Post Breast Surgery Risks,
Healing & Precautions
Your Body is Your Temple
Research, Resources & Education
Table of Contents
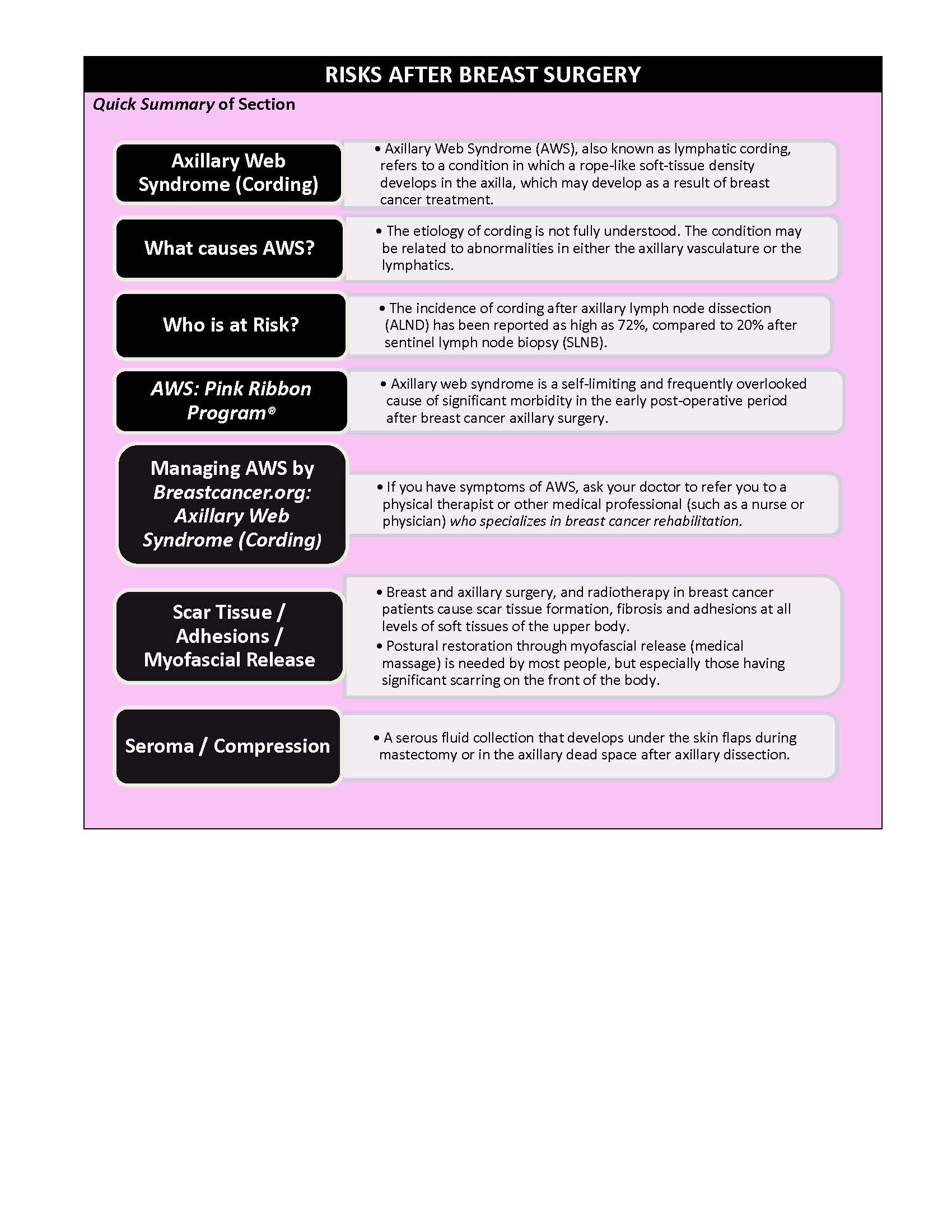
Breast surgery or a mastectomy can be a life-changing event for women. While these procedures may be necessary to address some health issues, it´s important to be aware of the potential risks involved. Among some of the risks that may arise after breast surgery or mastectomy are Axillary Web Syndrome (cording), seromas (fluid build-up), scar tissue or nerve damage.
Information and pictures from National Cancer Institute unless otherwise specified
Possible Complictions after Surgery Videos
YouTube Videos that help explain Possible Complications after Breast Surgeries, including Axillary Web Syndrome, Scar Tissue and Sermomas.
Disclaimer:
This is for research only and Lost Temple Fitness & Cancer does not endorse any video presented on this website.
It is advised that you ALWAYS CHECK WITH YOUR PHYSICIAN for a proper diagnosis and treatment plan.
Possible Complications after Breast Surgery
7 Videos
Axillary Web Syndrome - AWS (Cording)
Axillary Web Syndrome (Cording)
Axillary Web Syndrome (AWS), also known as lymphatic cording, refers to a condition in which a rope-like soft-tissue density develops in the axilla, which may develop as a result of breast cancer treatment.
- It usually appears in the 5 to 8 week period following breast cancer surgery and can lead to shoulder pain and restricted motion. (NCBI: PMC: Atypical presentation of axillary web syndrome)
- Cords are palpable bands of tissue which can occur in the axilla, across the antecubital fossa into the forearm and wrist, and in the breast or abdominal wall.
- The incidence of cording following breast cancer treatment ranges from 6 – 72%, and the condition can cause pain and limited range of motion in the upper extremity. (NCBI: PMC: Cording Following Treatment for Breast Cancer)
When does it happen:
- Typically 3-4 weeks post – op.
- Less often 2-4 weeks
- Less often over 4 weeks (Klose: Breast Cancer Rehabilitation)
Mondor disease is a rare condition that is characterized by scarring and inflammation of the veins located just beneath the skin of the chest.
- The affected veins are initially red and tender and subsequently become a painless, tough, fibrous band that is accompanied by tension and retraction of the nearby skin.
- In most cases, the condition is benign and resolves on its own; however, Mondor disease can rarely be associated with breast cancer.
- Although the condition most commonly affects the chest, Mondor disease of other body parts (including the penis, groin, and abdomen) has been described, as well.
- Mondor disease is thought to occur when pressure or trauma on the veins causes blood to stagnate.
- In most cases, the condition arises after recent breast surgery, but it can also be associated with physical strain and/or tight-fitting clothing (i.e. bras).
- Treatments are available to help relieve symptoms until the condition resolves. (NIH: NCATS: Mondor Disease)
What Causes AWS?
The etiology of cording is not fully understood.
- The condition may be related to abnormalities in either the axillary vasculature or the lymphatics.
- Anatomic studies of resected cords reveal that these structures may represent dilated and thrombosed lymphatics and/or thrombosed superficial veins.
- The condition is considered to be a variation of Mondor’s disease, a rare thrombophlebitis of the subcutaneous veins caused by trauma such as surgery. (NCBI: PMC: Cording Following Treatment for Breast) Cancer
- AWS: may be attributed to lymph venous injury during axillary lymph node dissection due to either tissue retraction and/or patient positioning.
- Another theory is that because of the interruption in axillary flow, lymphatic vessels are dilating and scalloping to the skin. (Summit Education: Oncology Rehab Dec 12, 2019)
Who is at Risk?
The incidence of cording after axillary lymph node dissection (ALND) has been reported as high as 72%, compared to 20% after sentinel lymph node biopsy (SLNB).
- Younger age, lower BMI, and being African-American have also been implicated as potential risk factors.
- While cording has been reported to cause limited range of motion, the extent to which this translates into dysfunction performing daily functional reaching activities has yet to be reported.
- Little data exists on whether cording is associated with an increased risk of developing upper extremity lymphedema. (NCBI: PMC: Cording Following Treatment for Breast Cancer)
Body habitus:
- Pt’s that have AWS were found to be more often of lower weight with a BMI between 23-25.
- Pt’s that were obese with a BMI between 26-28.9, unlike with lymphedema, tend to have a lower incidence of cording. (Klose: Breast Cancer Rehabilitation)
Axillary Web Syndrome by Pink Ribbon Program®
Axillary web syndrome is a self-limiting and frequently overlooked cause of significant morbidity in the early post-operative period after breast cancer axillary surgery, which is characterized by axillary pain that runs down the medial arm, limited shoulder range of motion affecting mainly shoulder abduction, and cords of subcutaneous tissue extending from axilla into the medial arm, made visible or palpable and painful by shoulder abduction.
- In addition, soft tissue may give a cordlike appearance due to increased tension between the skin of the upper arm and adherence of an axillary scar to underlying fascia.
- Lymphatic cording is associated with pain and limitation of shoulder movement, and it is common to find shoulder abduction restricted to less than 90°.
- Exercise interventions should typically include supine exercises involving assisted shoulder flexion, active abduction, horizontal abduction, and a trunk rotational stretch with shoulder abduction, stretching exercises for levator scapulae, upper trapezius, pectoralis major, and medial and lateral rotators muscles of the shoulder. (Pink Ribbon Program®)
Managing AWS by BreastCancer.org
If you have symptoms of AWS, ask your doctor to refer you to a physical therapist or other medical professional (such as a nurse or physician) who specializes in breast cancer rehabilitation.
- It’s not a good idea to wait and see if the condition will resolve on its own.
- Your natural reaction to the pain of cording will be to avoid moving the arm and shoulder, which can lead to more tightness in the shoulder and chest area.
- Over time, this may cause more serious problems with function and mobility.
- Moving and stretching under the guidance of an experienced therapist are the best ways to resolve the condition and stop the pain.
- Together, you and your therapist can develop a treatment plan that’s right for you. Your plan may include:
- Stretching and flexibility exercises: Your therapist can work with you to help you learn exercises that gently stretch the cords and improve your pain-free range of motion. He or she can teach you exercises to do at home and advise you on how often to do them.
- Manual therapy: Your therapist also may gently massage the cord tissue. Using manual therapy, your therapist would gently pull the tissue on your outstretched arm, starting in the upper arm and moving down into the forearm. This sometimes causes the cord to snap or break, and you may even hear a popping sound when that happens. It’s usually not painful, and it often brings relief by extending your arm’s pain-free range of motion.
- Moist heat: Your therapist may apply warm, moist pads directly to the cords as part of therapy. However, it’s important that he or she use caution when doing this. Prolonged heat can increase the production of lymph, which can lead to the fluid overload known as lymphedema. If your therapist recommends moist heat, just be sure he or she is experienced in its use for cording.
- Pain medication: You may need to take some form of pain medication, such as an NSAID (non-steroidal anti-inflammatory drug, such as Motrin or aspirin), if you experience pain that prevents you from stretching the arm. But remember that the best treatment for the pain is doing the stretching exercises that help the condition get better.
- Low-level laser therapy: Some therapists use a small, hand-held device to apply low-level laser beams directly to the skin. Laser therapy can help break down the hardened scar tissue.
- With the exception of pain medication, all of these treatments focus on releasing the tight scar tissue that makes up the cord(s).
- You may notice that releasing the cord in certain parts of the arm can magnify the tightness in other areas — not because the cording is getting worse, but because the scar tissue is still “stuck” in those other areas.
- For example, releasing the cord in the upper arm and elbow will reduce pain and improve range of motion, but the wrist and forearm may feel tighter at first.
- “I describe the cord to my patients as being like a fishing line that is stuck in several places along the fishing rod,” says Nicole Stout, MPT, CLT-LANA, physical therapist and lymphedema specialist, the Breast Care Center, National Naval Medical Center. “You can release a few of the stuck spots, but it then magnifies the tightness in the other areas that are still stuck.”
- Fortunately, cording usually resolves for most people after a few therapy sessions, or at least within a few months.
- It’s possible to have limited range of motion for many months or even longer, but that’s not typical.
- For some people, cording may get better and then come back later, but usually cording is a one-time event that doesn’t become a persistent problem.
- Experts still aren’t exactly sure what happens to the cords after they break down. Some experts believe that they simply get reabsorbed by the body, but other experts say that we simply don’t yet know what happens to the cords. (Breastcancer.org Axillary Web Syndrome (Cording)
Scar Tissue / Adhesions & Myofascial Release
Scar Tissue / Adhesions
An adhesion is a band of scar tissue that binds 2 parts of your tissue that are not normally joined together.
- Adhesions may appear as thin sheets of tissue similar to plastic wrap or as thick fibrous bands.
- The tissue develops when the body’s repair mechanisms respond to any tissue disturbance, such as surgery, infection, trauma, or radiation. (Web MD: Adhesions, General and After Surgery)
Breast and axillary surgery, and radiotherapy in breast cancer patients cause scar tissue formation, fibrosis and adhesions at all levels of soft tissues of the upper body.
- The occurrence or persistence of upper limb impairments after breast cancer treatment can partially be explained by the presence of myofascial dysfunctions (fascia surrounding and separating muscle tissue).
- Myofascial dysfunctions are expressed as myofascial trigger points and adhesions or restrictions of the myofascial tissues.
- The latter are impairments of gliding of the myofascial tissues relative to each other.
- Muscle manipulation during surgery, scar tissue formation, soft tissue adhesions and adaptive postures following surgery or fibrosis from radiotherapy can cause myofascial adhesions. (NCBI: An evaluation tool for Myofascial Adhesions)
According to Klose (K) and BreastCancer.org (B), tissue adhesion can cause:
- Pain (K)
- Postural changes (K)
- Impaired shoulder function (K)
- Movement compensations (K)
- Nerve pain or numbness if scar tissue forms around nerves. (B)
- A lump of scar tissue forms in the hole left after breast tissue is removed. If scar tissue forms around a stitch from surgery it’s called a suture granuloma and also feels like a lump. (B)
- Changes in breast appearance. Scar tissue and fluid retention can make breast tissue appear a little firmer or rounder than before surgery and/or radiation. (B)
Klose: Breast Cancer Rehabilitation (K) and BreastCancer.org: Scar Tissue Formation (B)
Myofascial Release
Postural restoration through myofascial release (medical massage) is needed by most people, but especially those having significant scarring on the front of the body.
- These scars draw the shoulders forward causing the head and neck to also pull forward. This leads to neck and shoulder aches and pains.
- The body is meant to be in alignment. When we live and move in non-optimal alignment, serious orthopedic injuries can occur.
- Most commonly, I have seen breast cancer survivors develop neck and shoulder impingement.
- Neck and shoulder impingement can cause shooting pain down the arm and lead to another surgery.
- Impingement syndromes start with achiness in the neck and shoulders.
- Myofascial release is a type of medical massage that is NOT painful.
- Focus is placed on gently releasing tension along thickenings of fascia and scar tissue.
- Releasing this tension restores posture and alignment.
- It also relieves knots and painful areas in all parts of the body.
Seromas & Compression
Seroma
A serous fluid collection that develops under the skin flaps during mastectomy or in the axillary dead space after axillary dissection.
- Incidence of seroma formation after breast surgery varies between 2.5% and 51% .
- Although seroma is not life threatening, it can lead to significant morbidity:
- Flap necrosis
- Wound dehiscence
- Predisposes to sepsis
- Prolonged recovery period
- Multiple physician visits
- May delay adjuvant therapy.
- Fluid collection is ideally managed by repeated needle aspiration to seal the skin flaps against the chest wall.
- Several factors have been investigated as the cause of seroma formation these include
- Duration of wound drainage
- Use of pressure garment
- Postoperative arm activity
- Preoperative chemotherapy
- Use of electrocautery (NCBI: Seroma formation after surgery for breast cancer)
Compression
Acute Management with Compression:
- Compression with pads and elastic garments
- Apply immediate compression after aspiration, when possible Seroma
Management Body Shapers:
- Avoid shelf bras
- Look for wide straps and good trunk coverage
- Breast cup vs. flat fabric design (depending on surgery
- Ensure coverage into the axilla
- Nighttime use if large breasted: daytime use if supportive enough to be used as a bra
- If currently on radiation, consult radiation oncologist (Klose: Breast Cancer Rehabilitation)
Post Healing Concerns After Surgery Videos
YouTube Videos that help explain different Post Healing Concerns after Breast Surgeries & Reconstruction.
Disclaimer:
This is for research only and Lost Temple Fitness & Cancer does not endorse any video presented on this website.
It is advised that you ALWAYS CHECK WITH YOUR PHYSICIAN for a proper diagnosis and treatment plan.
Post Healing Concerns after Breast Surgery
6 Videos
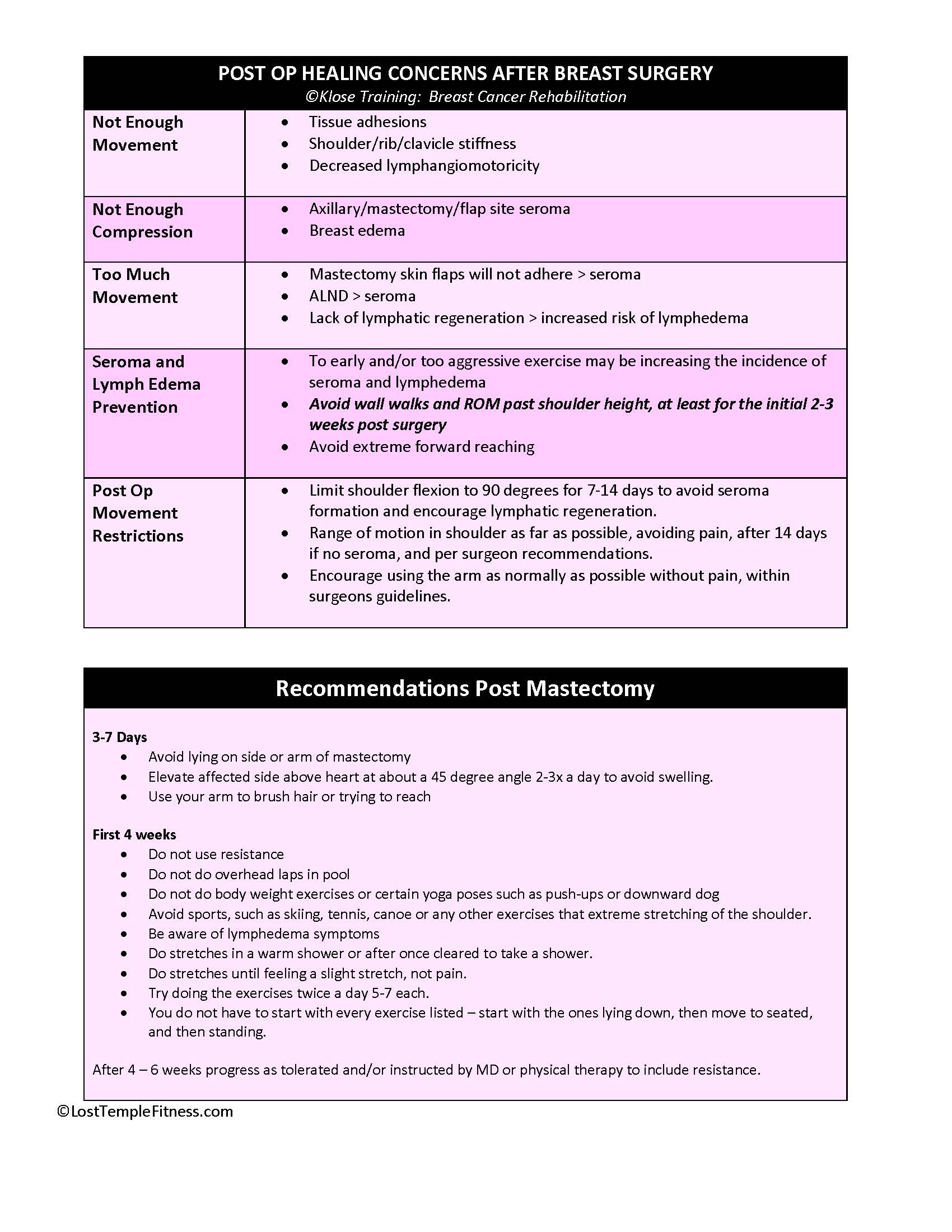
Post Healing Concerns 7 Recommendations After Surgery
Information from ©Klose Training: Breast Cancer Rehabilitation unless otherwise specified
- Tissue adhesions
- Shoulder/rib/clavicle stiffness
- Decreased lymphangiomotoricity
- Axillary/mastectomy/flap site seroma
- Breast edema
- Mastectomy skin flaps will not adhere > seroma
- ALND > seroma
- Lack of lymphatic regeneration > increased risk of lymphedema
- To early and/or too aggressive exercise may be increasing the incidence of seroma and lymphedema
- Avoid wall walks and ROM past shoulder height, at least for the initial 2-3 weeks post surgery
- Avoid extreme forward reaching
- Limit shoulder flexion to 90 degrees for 7-14 days to avoid seroma formation and encourage lymphatic regeneration.
- Range of motion in shoulder as far as possible, avoiding pain, after 14 days if no seroma, and per surgeon recommendations.
- Encourage using the arm as normally as possible without pain, within surgeons guidelines.
3-7 Days
- Avoid lying on side or arm of mastectomy
- Elevate affected side above heart at about a 45 degree angle 2-3x a day to avoid swelling.
- Use your arm to brush hair or trying to reach
First 4 weeks
- Do not use resistance
- Do not do overhead laps in pool
- Do not do body weight exercises or certain yoga poses such as push-ups or downward dog
- Avoid sports, such as skiing, tennis, canoe or any other exercises that extreme stretching of the shoulder.
- Be aware of lymphedema symptoms
- Do stretches in a warm shower or after once cleared to take a shower.
- Do stretches until feeling a slight stretch, not pain.
- Try doing the exercises twice a day 5-7 each.
- You do not have to start with every exercise listed – start with the ones lying down, then move to seated, and then standing.
After 4 – 6 weeks progress as tolerated and/or instructed by MD or physical therapy to include resistance.

Avoid for First Two Weeks after Surgery
Information from Cancer Rearch UK and Dana Farber unless otherwise specified
Your surgeon may suggest slightly different timings, so check if you are unsure.
- Don’t lift your arm above the height of your shoulder or stretch behind your back.
- Don’t lift anything heavier than a bag of sugar.
- You might not realize that some everyday things can strain your muscles. Avoid doing any of the following with your arm on the side of your surgery. Avoiding these things helps your muscles to slowly stretch and heal.
- Pushing yourself up off the bed
- Pushing doors open
- Pulling things towards you, such as pulling washing out of the washing machine
IMPLANTS
- The implant has been placed under the muscle at the front of your chest.
- It stretches the chest muscle more than usual.
- By avoiding the movements listed above, the implant won’t move and you won’t overstretch the muscle or the wound so it can all heal and settle down.
- When you are fastening your bra, do it up at the front, swivel it round, and put your arm on the side you had surgery in first.
- When you put your coat on, make sure you put the side you had surgery in the armhole first.
(Cancer Research UK)
If you have a lumpectomy or partial mastectomy with or without a sentinel lymph node biopsy:
- Avoid any activity that bounces or jostles the breast for two weeks after surgery (i.e.: running, jumping, using the elliptical machine).
- Perform shoulder range of motion as tolerated, beginning 1-2 days after surgery.
- If you have an axillary node dissection:
- You may want to use pillows to elevate your arm at night to decrease swelling during the first week.
- Putting a pillow between your arm and your side at night will prevent you from rolling on to the surgical site.
- You should avoid repetitive motions with the arm on the surgical side, such as vacuuming, for two weeks after surgery.
- Avoid heavy lifting for 4 weeks.
If you have a mastectomy without reconstruction:
- Perform shoulder range of motion as tolerated, even while the drains are in.
- You may return to low-impact exercises after surgery once your pain is controlled and you feel comfortable.
If you have breast reconstruction:
- You should not lift your arm above shoulder level until cleared by your plastic surgeon.
- You may return to low-impact exercises four weeks after surgery.
Walking is a great exercise to begin immediately to reduce bone loss, counter fatigue and nausea, and prevent muscle atrophy.
- After surgery, try to walk around for a few minutes 2-3 times per day.
If you’ve had a mastectomy do not lift your arm past shoulder level while the drains are in.
Disclaimer: The information in this book/website is for educational purposes only and has been obtained through research, publications and personal experience, and shall not be liable for incorrect information. Any mentioned publications or websites does not imply endorsement. As this industry is ever changing, I urge readers to confirm the information contained in this book/website. The author will not be liable for any injuries sustained from practicing techniques taught or for any typographical errors or omissions.
It is advised that you always check with your medical doctor or physical therapist before starting an exercise program or change in diet.
Information and pictures from National Cancer Institute unless otherwise specified